

by Jaclyn Long
figures by Tal Scully
A year into the pandemic, many people still struggle to get tested for COVID-19. By some estimates, asymptomatic transmission can account for up to 50% of all new cases, making regular testing of people who don’t yet (or might never) show symptoms a key part of a public health strategy to control the virus. Despite the effectiveness of mass testing, the US has failed to set up programs at scale, in part due to challenges such as the complex logistics, follow-up services, and infrastructure required for implementation. Even in settings where successful large-scale testing programs are in place, such as private universities, providing equitable access and identifying the ideal type of test remain key hurdles.
Multiple technologies can be used to detect the SARS-CoV-2 virus
There are two main categories of tests that can detect a current infection with SARS-CoV-2, the virus that causes COVID-19. Molecular tests, also called polymerase chain reaction (PCR) or viral RNA tests, leverage a technique called reverse transcription PCR. Using this technique, scientists can amplify and detect viral genes in a patient’s sample, most often taken from a nasal swab. These genes are not normally present in uninfected human cells, which make molecular tests very specific detectors for the active presence of the virus. The amplification steps of PCR allow scientists to detect even very small amounts of viral RNA, thus improving test sensitivity. The PCR itself is a fairly quick protocol, yielding results in a matter of hours. But the effective turnaround time of a test result can range from hours to days, depending on the laboratory facility where the test is processed. In some cases, it can take up to a week to obtain results, which limits the utility of these tests as a public health tool.
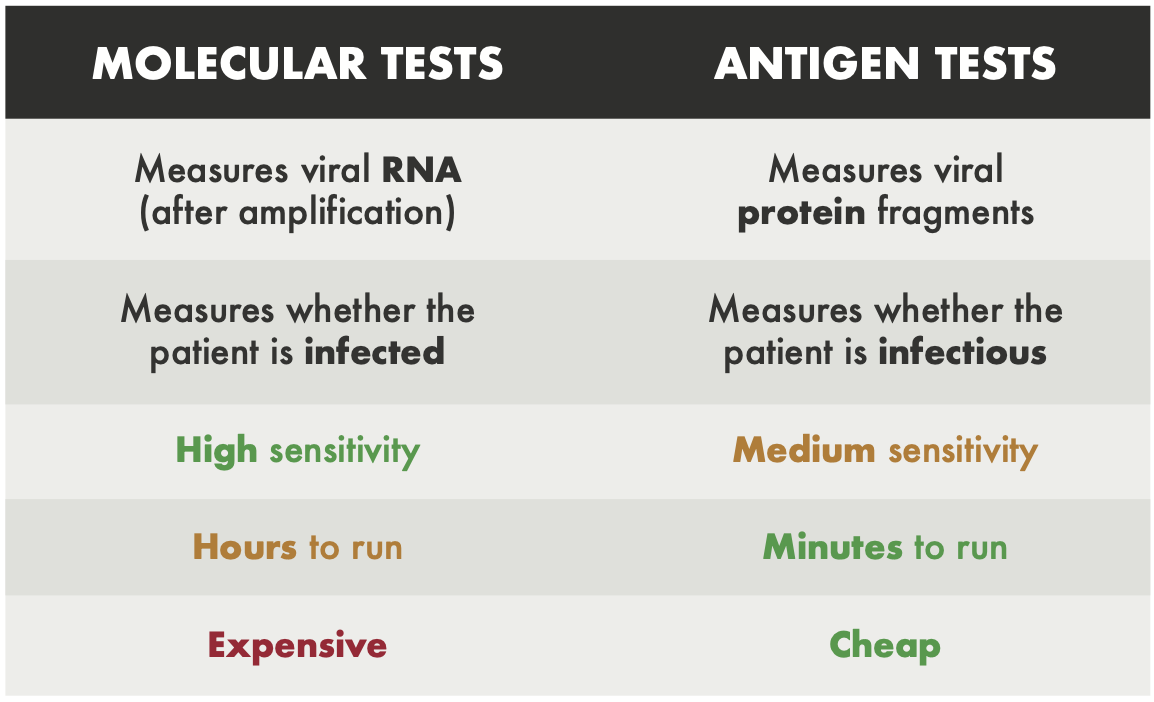
The other main category of diagnostic tests are antigen tests, also called rapid tests. These tests detect pieces of proteins that are found on viral particles, and so they are also highly specific. However, since they do not have an amplification step, antigen tests can only detect the viral protein if it is present at high levels in the patient’s sample. This means that these tests have a higher false negative rate than molecular tests, and might miss an active infection in a patient with low levels of virus. But antigen tests generally return an accurate positive result at the time when a person is most infectious, so these tests are still a valuable tool in curbing the pandemic. Importantly, antigen tests can be run very quickly and cost effectively without specialized equipment, often giving results in under 15 minutes. Many public health experts have argued that frequent, rapid tests would be a more effective tool to combat outbreaks than molecular tests with longer turnaround times.
Regular, asymptomatic testing requires complex logistics and resources
Of course, the tests themselves are only one piece of the COVID-19 testing puzzle. Regular, asymptomatic testing at a large scale also requires detailed logistical organization, numerous resources, and dedicated individuals and institutions. These often represent large barriers to implementation, particularly in lower income areas. Despite these hurdles, this kind of preventive testing has already been successfully implemented in many schools and universities across the country. Universities can therefore provide examples of the kind of infrastructure and investment that is necessary to perform asymptomatic testing on a large scale. To understand how Harvard University specifically identified and dealt with the hurdles of large-scale testing, I spoke to Dr. Giang Nguyen, the executive director of Harvard University Health Services (HUHS).
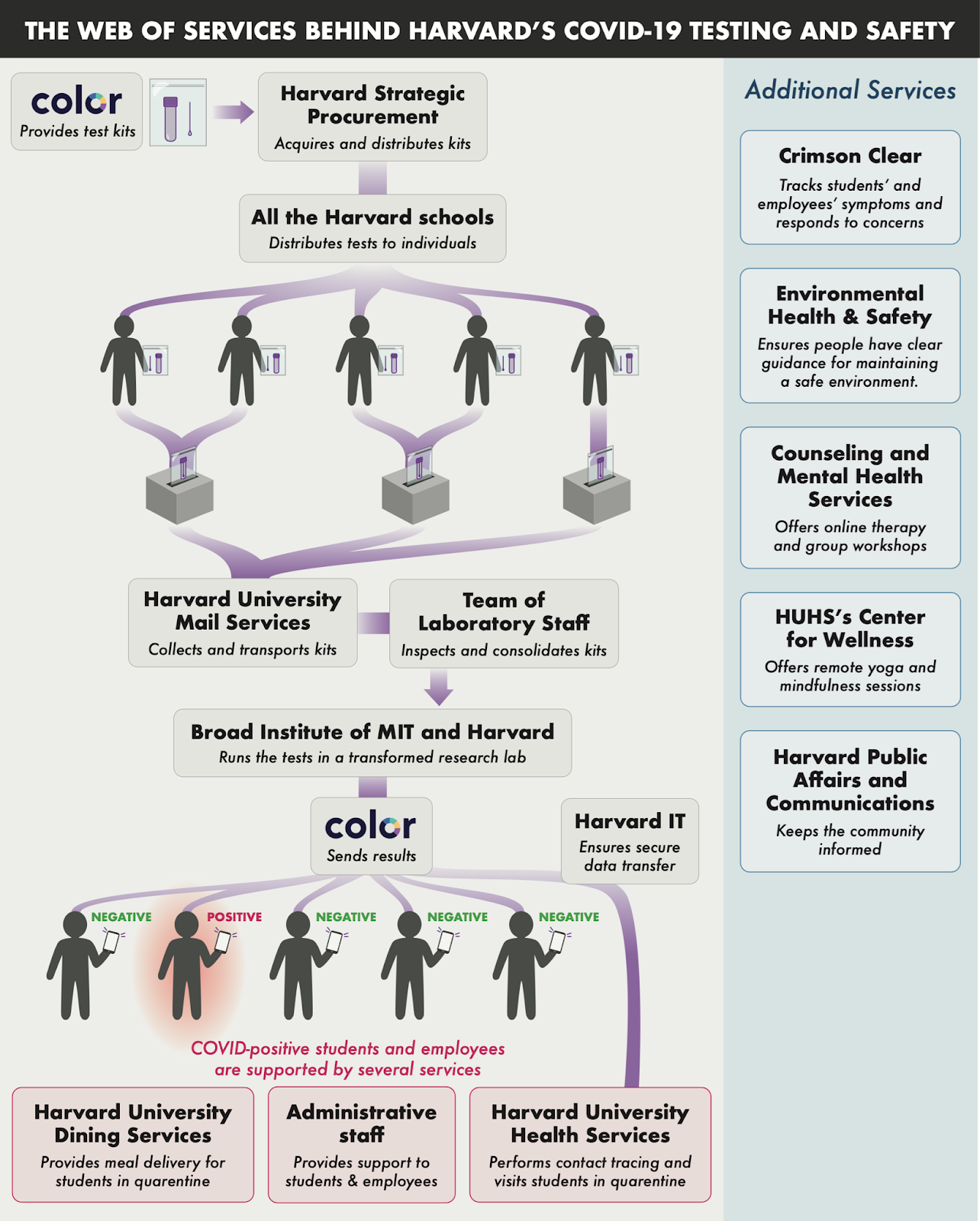
Harvard uses molecular tests, so their system requires laboratory space and equipment for them to be processed. In order to quickly establish such a space, the Broad Institute of MIT and Harvard transformed one of its laboratories into a large-scale COVID-19 testing facility early in the pandemic. Access to state-of-the-art technology and highly trained personnel enabled the Broad to quickly expand their capacity and process thousands of samples per day.
Dr. Nguyen explained that the testing process requires coordination across multiple services both within and beyond the university. The services involved include the genomics company Color, which manufactures and supplies tests, the Strategic Procurement group which distributes them throughout the university, Harvard University Mail Services to transport tests, and Harvard University IT to ensure that results are reported quickly and safely.
In addition to the many members of the community involved in the testing process itself, there is also an extensive network that is called into action when a test result comes back positive. These efforts help mitigate additional spread, since, as Dr. Nguyen notes, “testing doesn’t work if it is the only thing we do.” HUHS employees provide health care and contact tracing, administrative staff provide support for students through the disruptive process of quarantining, and Harvard University Dining Services provides meal delivery for students in isolation housing.
Harvard’s testing system, in combination with social distancing and masking measures practiced by the community, has prevented major outbreaks within the university. Dr. Nguyen pointed out that so far, their test positivity rates have remained under 1% (often well below 1%). He said that he is “hopeful that we will continue to see low positivity rates.” When laboratory equipment, investment from leadership, and support services are available, large-scale testing can be done in a way that protects the community. However, many communities lack the available infrastructure to implement testing at scale.
Equitable access to testing and services remains a major hurdle
At all levels, ensuring that testing is equitably available and accessible to all members of the community has been a significant challenge throughout the pandemic. When HUHS implemented unobserved self-administered testing in September, many contracted workers reported unequal access compared to similar employees directly employed by Harvard. Graduate students who work in hospital-affiliated Harvard labs were initially excluded from the testing program, despite peers in adjacent labs or simply on different payrolls with access. Postdoctoral researchers and staff who work in these settings are still not eligible for asymptomatic testing through Harvard.
But the issues with equitable access to testing are not confined within the Harvard community. In Massachusetts, for example, access to reliable testing remains inequitable. Students with access to programs such as Harvard’s can test regularly for free and generally receive results within 24 hours. In contrast, many members of the Boston community face confusing eligibility rules, steep prices, and long lines in order to get tested without showing symptoms. Testing deserts have been described throughout the U.S., and disproportionately impact vulnerable populations.
Outlook
Advances in technology have ensured that the presence of a SARS-CoV-2 infection can be detected accurately and rapidly. When identified in time and with proper measures, such as contact tracing and quarantining, an infection can be contained and the spread of the virus can be curbed. Scientists still debate over which tests are the most beneficial to use at a community-wide level. Regardless of the choice of test, however, the process of providing and managing testing at a large scale comes with numerous logistical hurdles. University-wide testing systems have taught us that broad, asymptomatic testing can work extremely well, but requires massive investment, coordination, and leadership. Even when all of these resources are available, we still need to carefully ensure that access to testing is equitable, and that no populations are left behind. These lessons should inform future pandemic preparedness in the aftermath of COVID-19.
Jaclyn Long is a first year Ph.D. student in the Immunology program at Harvard Medical School. You can find her on Twitter as @JaclynMLong.
Tal Scully is a third year Ph.D. student in the Systems, Synthetic, and Quantitative Biology program at Harvard University, where she studies zebrafish development and evolution. You can find her on Twitter as @TalScully.
Cover Image: “Covid-19 testing” by Prachatai is licensed under CC BY-NC-ND 2.0
For More Information:
- In May, we detailed the initial ramp-up of COVID-19 testing in the U.S.
- We also described a new antibody test that might help scientists understand the immune response to COVID-19
- We discussed some of the stark racial disparities in COVID-19.
- The FDA published additional information about the different types of COVID-19 tests
- Learn more about Harvard University’s testing strategy and COVID-19 testing in Massachusetts.
- Learn more about testing approaches in K-12 schools, including pooled PCR testing.