

by Beatrice Awasthi
figures by Tal Scully
Opioid use was a crisis in the United States long before the COVID-19 pandemic—among the 76,000 deaths due to drug overdoses in the United States between April 2019 and April 2020, at least 54,000 were caused by opioids (Figure 1). This represented a 12% increase in drug-attributed overdoses over the previous year. But the situation has grown even worse since the pandemic began, with at least 40 states seeing an increase in opioid-related deaths. The question is, how did the situation become so dire? What launched us into this crisis, why has it continued to worsen, and how might we begin to lower the rates of opioid use in the United States?

What are opioids?
Opioids are a class of compounds that bind to specialized receptors on nerve cells called opioid receptors. This binding process elicits a variety of effects, such as the blockage of pain signals and the stimulation of the body’s reward system. Some opioids, like endorphins, occur endogenously, or within the human body, while others, like morphine, are naturally occurring in plants. Certain opioid drugs, such as fentanyl, can also be synthesized artificially in a lab.
How efforts to manage pain led to an opioid crisis
Opioids have been used for pain management for over a century, but the opioid epidemic itself only began to develop in the 1980s – 1990s. It was at this time that the importance of pain management came into the spotlight. The American Pain Society labeled pain as “the fifth vital sign” and several states passed Intractable Pain Treatment Acts that permitted practitioners to use opioids to treat intractable pain in patients. Around the same time, it was widely publicized that opioids were not addictive or dangerous.
Today, it is known that this is far from true. Opioids are, in fact, highly addictive; one study found that 1 in every 10 to 11 patients will become addicted to opioids, while 1 in every 4 to 5 patients will misuse them. Prolonged use of opioids leads to the development of tolerance, meaning that higher doses are required to achieve the same effects of pain management, resulting in greater risk. At the same time, termination of an opioid prescription can lead to withdrawal symptoms, and the unpleasantness of withdrawal can present an additional challenge to controlling opioid consumption. Yet in the early days of the opioid epidemic, the marketing of opioids as a safe and effective way to relieve patients of pain resulted in a disastrous over-prescription of opioids that peaked in 2012—over 255 million opioid prescriptions were written that year. Though the number of opioid prescriptions in the United States has declined over the years as the direness of the situation has become clear, the prescription count remains high, with over 168 million given out in 2018.
Recently, many pharmaceutical companies are facing civil and criminal lawsuits for their role in exacerbating the opioid crisis through illicit marketing tactics. In November 2020, Purdue Pharmaceuticals pled guilty to illegally paying doctors to prescribe its opioid drug, OxyContin, and to paying the health records company Practice Fusion to send targeted messages encouraging increased opioid prescriptions to doctors. Several other drug companies are facing litigation for aggressive pro-opioid marketing as well. Recently, four drug companies that played a major role in supplying United States pharmacies with opioids—Johnson and Johnson, AmerisourceBergen, McKesson, and Cardinal Health—agreed to a tentative $26 billion settlement for their role in the opioid crisis. These companies were known to supply opioids to pharmacies at astonishing rates; between 2008 and 2018, for example, they shipped 20.8 million prescription painkillers to two pharmacies only four blocks apart in a West Virginia town with a population under 3,000.
Alternatives to opioids for pain relief
While opioids can be an effective treatment for pain, the efficacy of less-risky alternatives, such as non-opioid medications and physical therapy, should not be discounted. Studies have found that, in some cases, the effectiveness of non-opioid medications like acetaminophen in treating pain matched that of opioids. Additionally, physical therapy can be enormously helpful in treating some kinds of pain, and one cross-sectional analysis of patients with musculoskeletal pain found that early physical therapy intervention significantly reduced long-term opioid use. As a general rule, treatment strategies for treating pain should be specifically tailored to a patient’s case and the type of pain the patient is experiencing—pain is a complex, multifaceted issue that cannot be treated with a one-size-fits-all approach. And for certain types of pain, chronic opioid use may even make the pain worse.
Substantial evidence points to the effectiveness of interdisciplinary approaches to pain management (Figure 2). One study looking at patients with spinal cord injuries found that combining physical, occupational, recreational, and vocational therapy with pharmacologic medication that specifically targeted the root cause of pain significantly reduced patients’ need for opioid medication over several years. Such specifically targeted treatments included neuropathic medication to treat neuropathic pain and muscle relaxants to treat pain due to muscle spasticity. A different study examined the effects of acceptance and commitment therapy (ACT), a pain rehabilitation program that emphasizes pain education and both behavioral and physical strategies to increase patients’ ability to function despite their pain. This study found that ACT significantly improved patients’ pain severity, depressed mood, and ability to engage in life activities.
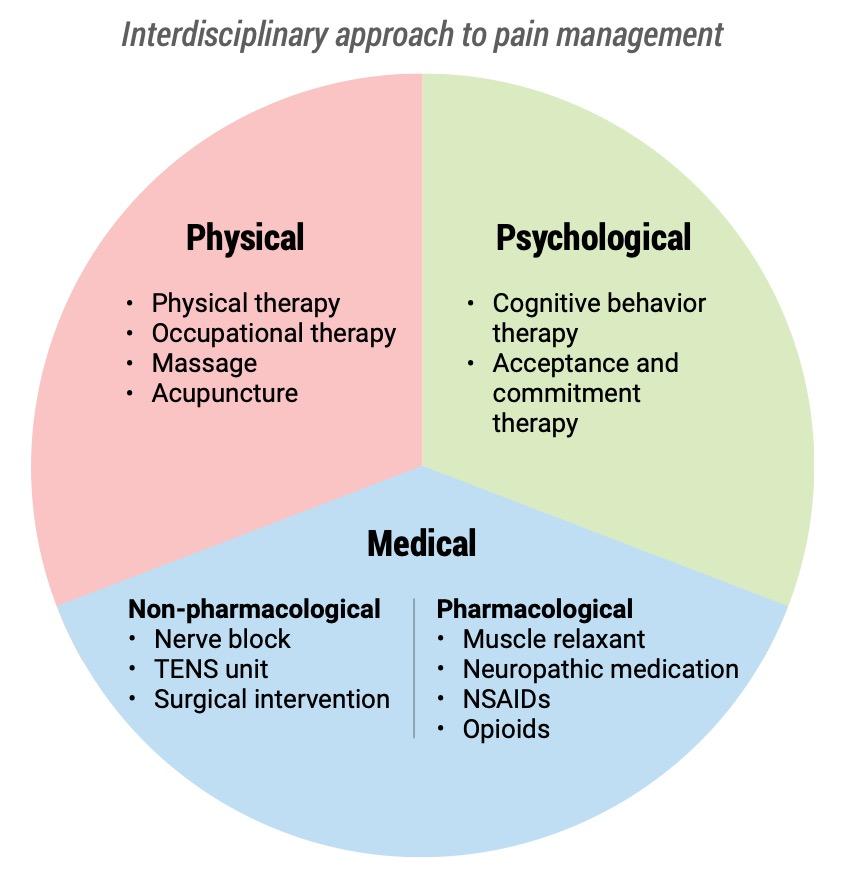
Interdisciplinary approaches to pain management have been found to be effective. Such multimodal treatment plans can include physical, psychological, and medical components.
How affordable is interdisciplinary pain management?
One hurdle to making interdisciplinary pain management approaches the norm is the level of financial commitment required upfront; hospitals and insurers may be reluctant to offer and reimburse such pain management programs due to apparent high costs of services required by chronic pain patients. Consequently, from a patient perspective, prescription opioids may be a substantially cheaper option than other modes of pain management. With insurance, the median out-of-pocket cost per patient per month was found to be only around ten dollars for prescription organoids, compared to approximately forty dollars for a single physical therapy visit. Yet, in the long-run, full commitment to a multidisciplinary pain management program might be substantially less of a financial burden on many levels. One economic study investigated the impact of an intensive interdisciplinary pediatric pain management program. It found that the structured pain management program could lead to thousands of dollars saved per patient for both hospitals and insurances due to a consequent reduction in hospital visits and hospital stays required due to pain. Moreover, the societal costs of prescription opioid abuse are staggering; they were estimated to be $55.7 billion in the United States in 2008, including healthcare costs of $25 billion. This evidence suggests that increasing the accessibility of interdisciplinary pain management programs to patients might be in the best interests of not only the patient, but of providers and insurers—not to mention society as a whole—as well.
Moving forward with pain management
Though it has been widely acknowledged that the opioid epidemic must be addressed—the Trump administration awarded large sums of money to combating the opioid crisis, and Joe Biden has announced his own plan to do so—practices in the United States still bolster opioid use. One NIH study found that around 21% of patients with musculoskeletal pain were prescribed opioids at their first doctor’s visit, even though the American Academy of Family Physicians recommends that multimodal treatments without an emphasis on medication should be considered as an initial line of treatment, with opioids only being recommended after non-opioid approaches have proven inadequate. Additionally, a simple opioid prescription to eradicate pain can seem like a simple, non-overwhelming path for patients. When pain strikes, it can be an exceedingly draining and lonely experience, especially if it is long-lasting. In some cases, the pain may prevent engagement in normal activities and hobbies, which can be frustrating, distressing, and lonely. It can be challenging—logistically, physically, and emotionally—to devote the time and energy to find a team to manage a pain condition, as it can require multiple attempts (and involve several unsuccessful ones) and extensive self-education.
Nevertheless, it is important to remember that there are many non-opioid options for treating various types of pain. Appropriate pain management for each patient should always be discussed with healthcare providers. Additionally, providers have the responsibility to look beyond opioids in situations where patients could be helped equally by an intervention that carries fewer risks. While these alternatives might require a greater up-front commitment, the increased quality of life, ability to engage in activities of choice, and avoidance of unnecessary risk are well worth it.
Beatrice Awasthi is a third-year PhD student in the Biological and Biomedical Sciences program at Harvard University, where she studies signaling in colon cancer.
Tal Scully is a third year Ph.D. student in the Systems, Synthetic, and Quantitative Biology program at Harvard University, where she studies zebrafish development and evolution. You can find her on Twitter as @TalScully.
Cover Image: “Pain Killers” by KJGarbutt is licensed under CC BY 2.0
For More Information:
- Though opioid use can be risky, many patients not only safely use them, but also depend on opioids to effectively manage their pain. This article describes how the opioid crisis has made it harder for these patients to get necessary opioid prescriptions.
- Check out this review to read more about the history of interdisciplinary pain management in the United States and its implications for the future. To learn more about specific interdisciplinary pain rehabilitation programs in the country, take a look at this focused review.
- For a comprehensive overview of the biology of addiction, check out this review.
- This review describes the origins of the opioid epidemic and potential solutions, which focus on medication-based strategies to combat the issue of addiction. Further opioid statistics can be found here and here. Additionally, this review highlights strategies for safe prescription opioid use.
I would hope you spend some time exploring / investigating Portugal’s drug laws and practices and why they are far more successful at reducing drug abuse, drug overdose deaths, and the illegal drug industry .
The medical community should be leading the effort to change our very punitive (and very racist) drug enforcement laws and to model the Portugal experience.
Our American drug treatment services are very inadequate, and the costs of our Drug Law enforcement far outweighs the costs of decriminalizing drug abuse, and vastly improving outpatient services.